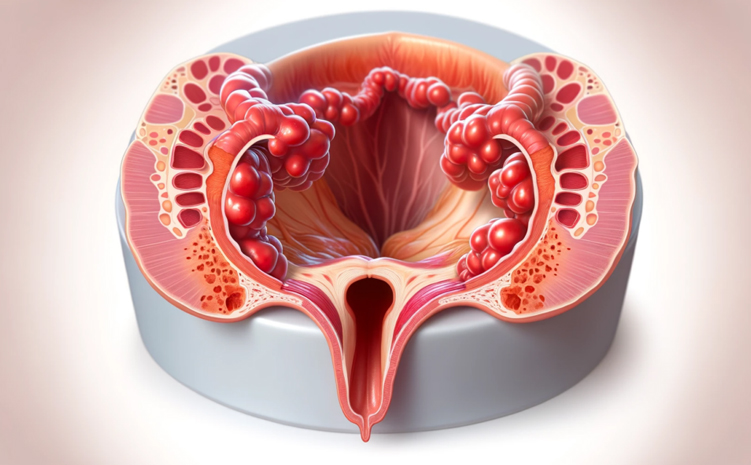
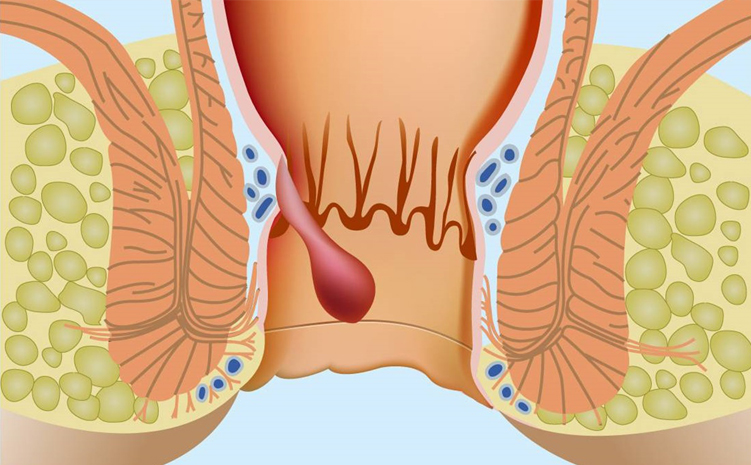
I know you are immediately thinking, "Well, sir, if these hemorrhoids are normal anatomical structures, why do they become symptomatic and become a disease?" To answer this question, we need to understand some anatomical structures simply. Imagine that there are arteries, veins and lymphatic channels in these packets in the 3-7-11 location on the clock dial, and these structures are covered with a red colored layer called mucosa on the anal canal wall, and there are internal muscle groups around the anus on the outside of the packets.
Imagine that these pads are attached to the inner muscle side with bands called Thomson ligaments in the inner part and Parks ligaments in the outer part. Imagine that these pads in their normal location in the anus are hanging out of the anus due to the rupture of these ligaments due to many reasons such as constipation and long-term straining. When you consider the weakness of the inner wall layer of these hemorrhoids and the edema in these packets due to straining, I think you understand that normal hemorrhoids turn into hemorrhoidal diseases that cause complaints. In other words, every person has "hemorrhoids", but when the existing hemorrhoidal anatomy is disrupted and the hemorrhoids hang down, hemorrhoidal disease occurs.
What is the frequency of hemorrhoidal diseases in the society?
Approximately 50% of the adult population encounters symptoms of hemorrhoidal disease at some point in their lives. (It should be emphasized that its frequency increases with age). Therefore, the disease is a serious health problem. If we talk about the seriousness of this health problem in terms of numbers; Approximately 120-150 thousand hemorrhoid surgeries are performed in America every year. If we include other treatment methods other than these surgeries in these figures, the rate is approximately 4% of the population. If we extrapolate these figures in our country, this means 30,000 surgeries and 2.8 million patients receiving treatment per year. This way, we will understand the burden of the disease on the social security system.
According to many studies, the age at which the disease becomes most symptomatic is between the ages of 45-65. More people believe that there is no difference in incidence between genders. However, it should be emphasized that pregnancy in women is often the period when the disease first becomes symptomatic.
What are the causes of hemorrhoidal disease?
Chronic diarrhea and constipation, chronic straining, pregnancy, hereditary factors, and occupational groups that stand for long periods of time are among the causes of hemorrhoidal diseases. Considering the role of long-term straining in etiology, regular defecation habits, which we will talk about later, are extremely important. It is a clinical fact that hemorrhoidal disease is more common in people with irregular bowel habits.
We know that white people are more affected than black people. Hereditary predisposition is extremely important. The disease frequency increases even more in those with advanced socioeconomic levels. Based on this statistical information, it is extremely effective in the formation of this disease (as we will explain in the nutrition section, as well as in the treatment steps of the disease). We can list the factors effective in disease formation as follows.
* Extends
* Anatomical features
* Nutrition
* Professions that require standing for long periods of time
* Advanced age
* Pregnancy
* Exercise
* Cough
* straining
* Vomiting
* Situations where intra-abdominal pressure increases
* Constipation
* Diarrhea
What complaints and findings do patients present with hemorrhoidal diseases?
Bleeding is the main symptom of hemorrhoidal diseases. Patients describe this bleeding as fresh red following defecation. They may describe this bleeding as smearing on toilet paper, dripping after defecation, or seeing blood in the toilet after defecation. In other words, bleeding is the leading complaint in hemorrhoidal diseases.
Apart from bleeding, another main symptom or finding of the disease is hemorrhoidal nozzles, which are palpable following defecation and which patients try to replace. As we mentioned in the anal fissure section, these skin folds called skintags in chronic anal fissures can be confused with hemorrhoid nozzles, and when the patient diagnoses hemorrhoids on his own, the crack may deepen due to treatment failure and loss of time.
The staging of the hemorrhoidal disease, which we will explain in the next section, is done according to whether these palpable hemorrhoidal breasts come out during straining, whether the protruding breast spontaneously re-enters the anus, or whether these breasts can only be inserted back into the anus manually or cannot be inserted into the anus manually in any way.
Some patients may experience itching and a feeling of wetness due to the irritating properties of the secretions of protruding hemorrhoid nozzles on the anal area skin. It should also be kept in mind that this sagging may cause hygiene problems by causing stool contamination in the patient's underwear.
It is generally accepted that there is no pain complaint in hemorrhoidal diseases. The presence of a complaint of pain primarily brings to mind an anal fissure disease that may occur simultaneously with hemorrhoids. Pain complaints will occur in the advanced stages of the disease, that is, when the hemorrhoid nozzles sag outwards.
Severe throbbing pain occurs when clots form inside the hemorrhoidal breasts, called thrombosed hemorrhoids. This pain usually starts suddenly following a difficult defecation.
To emphasize an important point here; The anal region is a localization where many different types of pain occur due to many reasons, and it should be known by both the physician and the conscious patient group that there may be a group of unhappy patients whose pain is attributed to hemorrhoids and whose pain continues despite surgery, but the real underlying cause is overlooked.
It is extremely important for the patient to remain calm with a sense of mutual trust with the physician in order to avoid missing additional underlying problems due to inadequate evaluation of the anal area, as patient privacy is at the highest level during the proctological examination, and the patient's sense of embarrassment may be triggered by the pain that may occur during the examination.
Grading and naming in hemorrhoidal disease
If you imagine the anal canal as a cylinder, anatomically approximately 4 cm long, imagine a horizontal line passing through the middle of this canal. This bed line is the dentate line. You now know that hemorrhoids located above this line, that is, deeper, are called internal hemorrhoids, and hemorrhoids located outside the line are called external hemorrhoids. Now imagine that while internal hemorrhoids are in their normal anatomical structure above the dentate line, the vascular bundle inside begins to sag outward as the ligaments that fix it to the internal muscle wall are broken each time with difficult straining. This is how internal hemorrhoids are divided into four groups.
1st degree internal hemorrhoids;
The hemorrhoid nozzle is above the dentate line, and the hemorrhoid nozzle cannot be seen from the outside even if the patient strains.
2nd degree internal hemorrhoids;
The hemorrhoid nozzle comes out of the anus when the patient strains. It goes back in after straining.
3rd degree internal hemorrhoids;
Hemorrhoid nozzles are exposed during defecation. These breasts, which cannot be inserted by straining, can only be inserted by the patient's manual intervention.
4th degree internal hemorrhoids;
Hemorrhoid nozzles are always outside in the anus. It will come out more during straining and defecation. It is not possible to insert the hemorrhoid nozzles even by hand.
As we explained above, hemorrhoidal disease is thought to start in the inner part of the anus and progress by sagging outwards. However, in some cases, they are called external hemorrhoids because they may be outside the anus, just below the dentate line, even though there is not much disease inside. In terms of localization, external hemorrhoids are more painful.
It should be known that both internal and external hemorrhoids can occur in the same patient. These are called mixed type hemorrhoids.
How to examine the patient and diagnose hemorrhoidal disease?
At the time of admission, after the physician carefully learns the history from the patient, it is appropriate to perform the proctological examination of the patient, ideally on electric proctology tables. Patient privacy should be given importance here.
The examination begins with observation of the anal area. Here, the physician must rule out anal fissure (anal fissure) disease, which is extremely important for differential diagnosis in the anal area. We proceed to evaluate the findings, which we will explain in detail in the anal abscess/anal fistula section. It may be possible to see hemorrhoidal pockets that may be provoked by the patient straining. Additionally, Grade 4 internal hemorrhoid nozzles or thrombosed (clotted) external hemorrhoid pecs may be seen outside.
By establishing communication with the patient, manual examination is started. Evaluating the area around the anus with a finger is important in terms of sensitivity and anal abscess. It should be evaluated whether there is redness (hyperemia) around the anus.
During the rectal examination, the physician evaluates the hemorrhoids using the finger. Internal hemorrhoids can be graded by straining, if necessary.
There are two very important points that must be evaluated during anal examination. The first of these is the prolapse of the innermost layer of the intestine, called rectal prolapse, during straining, and the other is the rough evaluation of the pressure of the anal region muscles at rest and contracting the anus.
We need to share extremely important information in this section. Hemorrhoid breasts never become cancerous. However, it should be kept in mind that in cases where the most important complaint is bleeding, this symptom may be due only to hemorrhoidal disease, and the underlying colon cancer may be missed. Therefore, in patients who apply with rectal bleeding, the age of the patient is important, and it is important to question the patient's complaints such as family history, weight loss, fatigue, constipation in terms of colon cancer, and to perform an endoscopic examination if necessary.
It is scientifically known that approximately 3% of patients under the age of 40 and 11% of patients over the age of 40 who present with rectal bleeding may have underlying cancer and other important pathologies.
Important diseases in differential diagnosis that may be confused with hemorrhoidal disease
Three important diseases should be kept in mind in differential diagnosis.
1.Anal incontinence with or without prolapse
2.Anal fissure disease
3. Colon cancer
Anal region and rectum cancers are undoubtedly the most important diseases in differential diagnosis. Many anal region cerectum cancer patients can receive treatment for hemorrhoids for a long time either on their own or as a result of evaluation by pharmacists and inexperienced physicians. In fact, this problem exists all over the world. In the famous medical book Cameron, it is reported that the rate of rectal cancer patients in the USA thinking they have hemorrhoids is 52%.
In summary, hemorrhoids do not become cancerous; they may overshadow the underlying cancer in the differential diagnosis.